Education
Exposure of Left Brachial Plexus
Position - supine with small transverse shoulder roll to allow slight extension of the head and neck. The head is placed on a donut headrest and rotated approximately 50 degrees to the right.
 Incision - The incision is scored with a no. 15 blade along the posterior border of the sternocleidomastoid (SCM) from just below the ear to just above the head of the clavicle.
Incision - The incision is scored with a no. 15 blade along the posterior border of the sternocleidomastoid (SCM) from just below the ear to just above the head of the clavicle.
It is taken sharply through the level of the dermis after which a micropoint cautery (cut 6, coag 8, blend 1, standard) is used to divide the subcutaneous fat and platysma.
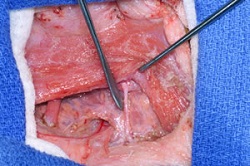
 Dissection - The dissection begins by separating a lateral myocutaneous flap from the posterior border of the SCM. The spinal accessory nerve is identified at the posterior border of the SCM coursing across the posterior cervical triangle. Just caudal to the accessory nerve, cutaneous branches of C4 are seen emerging from the supraclavicular fat/nodal tissue. A vein often accompanies these cutaneous branches.
Dissection - The dissection begins by separating a lateral myocutaneous flap from the posterior border of the SCM. The spinal accessory nerve is identified at the posterior border of the SCM coursing across the posterior cervical triangle. Just caudal to the accessory nerve, cutaneous branches of C4 are seen emerging from the supraclavicular fat/nodal tissue. A vein often accompanies these cutaneous branches.
Between the cutaneous branches of C4 and the clavicle, the inferior belly of the omohyoid is identified and freed of investing fascia.
The supraclavicular fat/nodal tissue is divided vertically along the medial margin of the lateral myocutaneous flap and reflected medially up off of the plexus, preserving its association with the jugular chain of nodes and venous drainage.
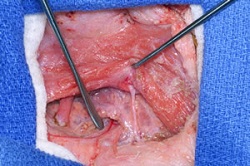
The omohyoid is reflected caudally during this maneuver to further exposure the portion of the plexus immediately proximal to the clavicle.
 Note the internal jugular vein, and anterior and middle scalene muscles in the figure at right. The apex of the scalene triangle is consistently found just below the point of emergence of the C4 cutaneous branches. Several branches to the phrenic nerve are seen crossing the anterior scalene.
Note the internal jugular vein, and anterior and middle scalene muscles in the figure at right. The apex of the scalene triangle is consistently found just below the point of emergence of the C4 cutaneous branches. Several branches to the phrenic nerve are seen crossing the anterior scalene.
In this example, a large neuroma is seen occupying the supraclavicular fossa.